

Diabetic shock is a state of severe low blood sugar, known medically as hypoglycemia, that occurs when blood glucose levels plunge dangerously below the normal range. Insulin shock is an older medical term that describes the exact same condition. Both terms refer to severe hypoglycemia a medical emergency in which the brain and body do not receive enough glucose to function properly.
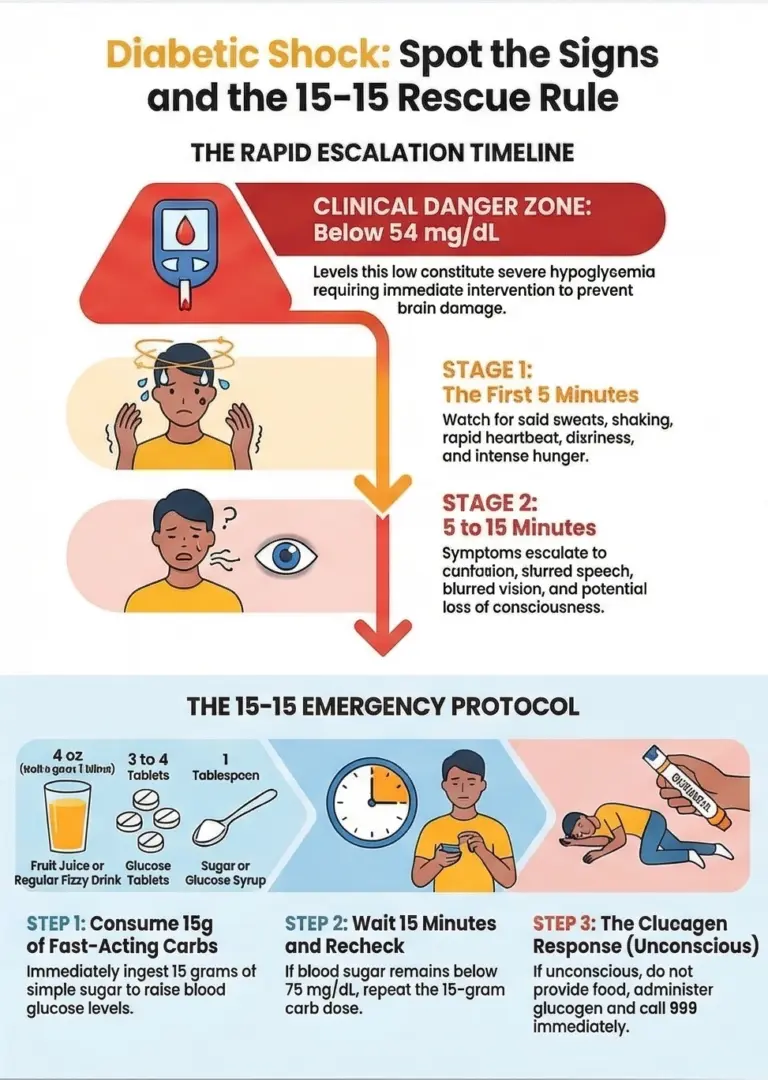
According to the American Diabetes Association (ADA), blood glucose below 70 mg/dL is considered clinically significant, and levels below 54 mg/dL constitute severe hypoglycemia that demands immediate action. Without prompt treatment, diabetic shock can progress to seizures, diabetic coma, and can be fatal.
This guide explains the difference between these commonly confused terms, walks through symptoms stage by stage, and provides the exact 15-gram treatment protocol endorsed by leading diabetes organizations.
TL;DR
- Diabetic shock and insulin shock are two names for the same life-threatening emergency: severe hypoglycemia, defined as blood glucose below 54 mg/dL.
- Symptoms progress from sweating and shaking to confusion, seizures, and loss of consciousness within minutes.
- The treatment is immediate: consume 15 grams of fast-acting carbohydrates, wait 15 minutes, and recheck blood sugar.
- If the person is unconscious, administer glucagon and call 911.
- Left untreated, diabetic shock can lead to diabetic coma and, in rare cases, death.
The Big Confusion: “Diabetic Shock” ≠ What You Think
One of the biggest sources of confusion around diabetic emergencies is terminology. When most people search for “diabetic shock,” they are referring to what medical professionals call severe hypoglycemia dangerously low blood sugar.
Similarly, “insulin shock” is an outdated clinical term from the early days of insulin therapy, but it describes the same condition.
According to the Cleveland Clinic, hypoglycemia occurs when blood glucose drops below the range that is healthy for you and severe cases can be life-threatening without treatment.
Meanwhile, “hyperglycemic shock” is not a recognized medical diagnosis. People who use that phrase are typically thinking of diabetic ketoacidosis (DKA) or hyperosmolar hyperglycemic state (HHS) both high blood sugar emergencies with blood glucose levels often exceeding 600 mg/dL.
These are the opposite of diabetic shock and require entirely different treatment, usually intravenous insulin in a hospital setting.
| Term People Google | Actual Medical Term | Blood Glucose Level |
| Diabetic shock | Severe Hypoglycemia | <54 mg/dL |
| Insulin shock | Severe Hypoglycemia | <54 mg/dL |
| Hyperglycemic shock | DKA / HHS | >600 mg/dL |
Critical: From the first signs of confusion, a person experiencing severe hypoglycemia can progress to seizures, brain damage, and death within 15 minutes if left untreated. This is why recognizing the warning signs and acting immediately is essential for every person with diabetes and their family members.
Insulin Shock Symptoms: 5-Minute → 15-Minute Timeline
Diabetic shock symptoms develop rapidly and escalate in severity. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) notes that symptoms usually appear when blood sugar levels fall below 70 mg/dL and can quickly become dangerous. Recognizing these warning signs early is the key to preventing a life-threatening emergency.
Stage 1 Early Warning Signs (Blood Glucose 70-54 mg/dL, first 5 minutes)
- Sweating (cold, clammy skin)
- Shaking and tremors
- Rapid heartbeat (tachycardia)
- Intense hunger and irritability
- Dizziness and lightheadedness
Stage 2 Severe Symptoms (Blood Glucose <54 mg/dL, 5-15 minutes)
- Confusion and inability to concentrate
- Slurred or trouble speaking (may mimic a stroke)
- Difficulty walking and poor coordination
- Blurred or double vision
- Seizures, loss of consciousness, and coma
| Timeframe | Symptom | Recommended Action |
| 0-5 min | Sweating, shaking, hunger | Consume 15g carbs immediately |
| 5-15 min | Confusion, slurred speech, seizures | Administer glucagon kit |
| 15+ min | Unconscious, unresponsive | Call 911 + administer glucagon |
Some people may not experience the typical symptoms of hypoglycemia a condition called hypoglycemia unawareness.
According to the NIDDK, approximately 25% of people with type 1 diabetes experience this condition, making continuous glucose monitoring especially important for detecting blood sugar drops before they become dangerous.
15-Second Treatment: The 15g Rule
The standard emergency protocol for treating low blood sugar is called the 15-15 rule, recommended by the ADA and the CDC. It involves consuming 15 grams of fast-acting carbohydrates to raise blood glucose levels, waiting 15 minutes, and then rechecking blood sugar levels.
If blood glucose levels remain below 70 mg/dL after 15 minutes, another 15 grams of fast-acting carbohydrates should be consumed. Once blood sugar returns to the target range, eat a balanced snack or meal with protein and complex carbohydrates to stabilize levels.
For a conscious person:
- Check your blood sugar if possible.
- Consume 15 grams of fast-acting carbohydrates immediately.
- Wait 15 minutes and recheck blood sugar.
- If still below 70 mg/dL, repeat. Once stabilized, follow up with complex carbs (e.g., peanut butter crackers).
| 15g Fast-Acting Carbohydrate | Portion Size |
| Orange juice or fruit juice | 4 oz (half a glass) |
| Glucose tablets | 3-4 tablets |
| Glucose gel | 1 tube |
| Regular soda (NOT diet) | ½ cup (4 oz) |
| Sugar or corn syrup | 1 tablespoon |
| Hard candies | Check label for 15g |
For an unconscious person (glucagon emergency):
If someone experiencing a diabetic emergency loses consciousness, do not attempt to give food or drink as this may cause choking. Instead, position the person safely on their side to keep the airway clear.
- Glucagon nasal spray (Baqsimi): Administer 1 spray into one nostril. Effective within 10-15 minutes. No reconstitution needed.
- Glucagon injection (GlucaGen): Inject into the thigh. Effective within 5-10 minutes.
- Call 911 immediately. Hospital treatment may include IV dextrose as a backup.
The treatment for severe hypoglycemia is an injection of glucagon, which causes the liver to release sugar into the blood. Inform family members and friends about where to find glucagon and how to administer it the ADA emphasizes that an individual does not need to be a healthcare professional to safely give glucagon.
Causes: Why Insulin Shock Happens
Diabetic shock can be triggered by several factors, and understanding these risk factors is essential for diabetes management. According to the NIDDK, low blood sugar is most common among people who take insulin, but it can happen to anyone on certain diabetes medicines.
Top 5 Triggers:
- Too much insulin: Taking more insulin than needed can cause blood sugar levels to drop too low. Dosing errors with medications like Novolog or Lantus are a common cause.
- Skipped or delayed meals: Hypoglycemia can happen if you eat less than usual after taking diabetes medicine. The body breaks down food into glucose, and without that intake, blood sugar drops.
- Excessive physical activity: Exercising more than usual after taking diabetes medicine can lead to low blood sugar, as muscles consume more glucose during activity.
- Drinking alcohol: Alcohol interferes with the liver’s ability to release stored glucose, which can cause blood sugar to drop unpredictably.
- Medication errors: Sliding-scale insulin dosing, especially in long-term care settings, and dose-escalation with newer medications can lead to unexpected lows.
| Risk Group | Common Cause | Prevention |
| Type 1 Diabetes | Pump failure / dosing error | CGM alarms, backup supplies |
| GLP-1 users (new) | Appetite suppression → skipped meals | Snack schedule, lower initial dose |
| Nursing home residents | Sliding scale insulin errors | Basal-bolus protocol |
People with type 1 diabetes are most at risk of diabetic shock, but anyone living with diabetes can experience it especially those on insulin therapy or sulfonylureas.
Diabetic Shock vs Hyperglycemia: Don’t Mix Them Up
One of the most dangerous mistakes in a diabetic emergency is confusing low blood sugar with high blood sugar. These are opposite emergencies that require completely different treatments. Giving insulin to someone who is already in diabetic shock (low blood sugar) can be fatal.
| Insulin Shock (Low BG) | DKA / HHS (High BG) |
| Blood glucose <54 mg/dL | Blood glucose >600 mg/dL |
| Rapid onset (minutes) | Gradual onset (hours to days) |
| Sweating, confusion, shaking | Extreme thirst, nausea, fruity breath |
| Treatment: juice, glucose, glucagon | Treatment: IV insulin at hospital |
| Can be resolved in ~15 minutes | Requires hospital admission |
Quick test: Sweating + confusion = likely LOW blood sugar (give juice). Extreme thirst + fruity-smelling breath = likely HIGH blood sugar (call 911). When in doubt, check blood glucose levels with a meter or continuous glucose monitor and seek immediate medical attention.
Glucagon Emergency Kit: Every Person with Diabetes Needs One
The ADA Standards of Care recommend that glucagon be prescribed to anyone using insulin or at high risk for hypoglycemia. Newer formulations, such as the Baqsimi nasal spray, do not require reconstitution, can be stored at room temperature, and have a two-year shelf life making them far more practical than older injectable kits.
Who should carry a glucagon kit:
- All insulin users (type 1 and type 2 diabetes on Lantus, Novolog, or pump therapy)
- People starting GLP-1 medications (first 4-8 weeks carry elevated risk)
- Nursing home residents on insulin, per clinical guidelines
It is important to educate family and friends about the symptoms of hypoglycemia and to inform them about where to find glucagon and how to administer it in case of an emergency. A medical alert bracelet can also inform emergency personnel that a person has diabetes, enabling faster and more appropriate care.
GLP-1 / Ozempic Users: Elevated Risk in the First Weeks
Newer GLP-1 receptor agonists such as semaglutide (Ozempic) can increase hypoglycemia risk during the initial dose-escalation period, particularly when combined with insulin or sulfonylureas. The mechanism involves appetite suppression leading to skipped meals, delayed gastric emptying causing unpredictable glucose absorption, and dose escalation that may outpace the body’s adjustment.
Prevention tips for new GLP-1 users:
- Eat small, regular meals or snacks every 3 hours, even if appetite is reduced
- Set continuous glucose monitor alarms for readings below 80 mg/dL
- Keep a glucagon kit at the bedside during the first 4-8 weeks
- Discuss insulin dose adjustments with your healthcare provider before starting a GLP-1 medication
If a person has symptoms of hypoglycemia several times a week, they should see their healthcare professional to possibly change their diabetes treatment plan.
Prevention: How to Avoid Diabetic Shock
Preventing diabetic shock starts with careful diabetes management and awareness. The following strategies, supported by the ADA and the NIDDK, can significantly reduce the risk of severe hypoglycemia:
- Monitor blood glucose levels regularly: A person should check blood glucose levels regularly to prevent diabetic shock. Use a blood glucose meter or continuous glucose monitoring system to detect if blood sugar levels drop too low.
- Eat regular meals: Eating regular meals and snacks throughout the day helps maintain stable blood sugar levels. Never skip meals, especially after taking diabetes medicine.
- Adjust targets with your healthcare team: People can adjust their blood sugar targets according to their individual needs, especially those with hypoglycemia unawareness.
- Carry fast-acting carbohydrates at all times: Keep glucose tablets, fruit juice, or regular soda accessible to treat low blood sugar levels quickly when they occur.
- Wear a medical alert bracelet: This can inform emergency personnel that a person has diabetes and help ensure appropriate treatment.
- Educate family and friends: Teach family members, friends, and coworkers about the symptoms of hypoglycemia and where to find and how to administer glucagon in an emergency.
- Adjust for physical activity and alcohol: Plan carbohydrate intake around exercise, and be cautious with alcohol, as drinking alcohol can block the liver’s glucose release.
Disclaimer: This information is intended for general knowledge and informational purposes only and does not constitute medical advice. Always consult with a healthcare professional for personalized guidance.
Written by the Pandameds.com Editorial Team
Our content is created by pharmacy-trained researchers and healthcare specialists and rigorously reviewed by a diverse panel of authentic experts from the pharmaceutical and healthcare fields. This collaborative review process ensures that every article meets the highest standards of medical accuracy, reliability, and relevance.
- ✅ Authored by pharmacy-trained professionals
- 🔍 Reviewed by multiple verified experts in the pharmaceutical and healthcare niche
- 💊 Based on trusted sources including FDA, Health Canada, and peer-reviewed clinical studies
- 🔄 Regularly reviewed and updated every 90 days to maintain accuracy and trustworthiness
About Pandameds.com
Pandameds.com is a prescription referral service and help U.S. patients to access affordable and authentic weight loss medications.
Fast, Reliable Shipping to the USA!
Affordable Prescription Meds From Canada






Join our mailing list for exclusive promos, curated health content & more.
Related Blog Posts

Call Us Today!
If you have any questions, please email our support team at support@pandameds.com or call us toll-free at 1-888-862-1210.


